
On June 12, 2020, there was a “near miss” incident where two trains could have, but did not, have a sideswipe collision just south of Osgoode Station. The was first reported in the Toronto Star by Ben Spurr on June 4, 2021 (the linked article is behind the Star’s paywall).
Immediately this spurred several questions including “how could this happen” and “why did the TTC Board only learn of this through the newspapers almost a year after the fact”.
TTC management launched an external review of the incident, and the report from it is dated February 3, 2021. Management planned to bring a report to the Board in September 2021. A partly redacted version of the external review has been published by the TTC. Portions are omitted for reasons of confidentiality as permitted by the City of Toronto Act.
This report is about labour relations or employee negotiations.
This report is about litigation or potential litigation, including matters before administrative tribunals.
Osgoode Interlocking Incident Report, p. 1
What Happened?
A northbound train (run 114) at St. Andrew Station was held due to an on-board emergency. In order to maintain service on the University-Spadina leg of Line 1, the TTC directed a southbound train (run 123) at Osgoode to short turn via the pocket track south of the station.
Although this track is not often used, this type of move is common at several locations on the subway network during emergency turnbacks or when a line is split for construction projects.
An important distinction with Osgoode pocket track is that it ends in a blank wall north of St. Andrew Station. Unlike other locations with centre tracks such as the one between St. Andrew and Union, or those on Line 2 between Broadview and Chester, or beween Ossington and Christie, this track dead ends and can only be entered from one direction.
For reasons that are not yet clear, the Automatic Train Control system (ATC) (which had already been operational in this part of Line 1 for a few months) did not work, or was not used by trains entering the pocket track, and they did so under manual control.
The correct operating procedure was for a train leaving the pocket to switch back to ATC mode so that its move onto the mainline would be managed and protected by the signal system. This was not done, and when run 123 left northbound under manual control there was a conflicting move by train 114 which had by then left St. Andrew Station under ATC. There was no mechanism for the ATC system to detect the potential conflict between the trains.
The guard at the rear end of run 123 saw run 114 passing by on the mainline, and alerted the operator at the head of the train. He stopped run 123 5.8 metres away from run 114.
This incident arose through a combination of events and design:
- ATC either did not work, or was not routinely activate for movements into the pocket track.
- Manual operation of trains in ATC territory is very rare and should be done with maximum supervision to ensure there are no conflicting movements. When there is an emergency, supervisory attention could be divided among multiple activities.
- The train stopped in the pocket track clear of the switches, but the signal indicating if a route out of the pocket was clear was beside the train and not visible to the operator.
- There was confusion by the operator of the train about whether he had clearance to proceed out of the pocket track. Line 1 is in transition between operating modes with different indications by signals and console displays depending on the location and whether a train is in manual or automatic mode.
- The track layout makes it possible for a train to drive manually out of the pocket toward the northbound platform even though the route was not actually clear.
The diagram below (excerpted from the external report) shows the track layout for a train moving into the pocket. Switches 5B and 5A are aligned for movement between the southbound platform and the pocket. There is a sign at the south end of the pocket track indicating where trains should stop, but it is possible to be clear of the 5A switches without reaching this point. However, if the train stops north of that sign, signal X8 could be beside the north end of the train rather than in front of it.
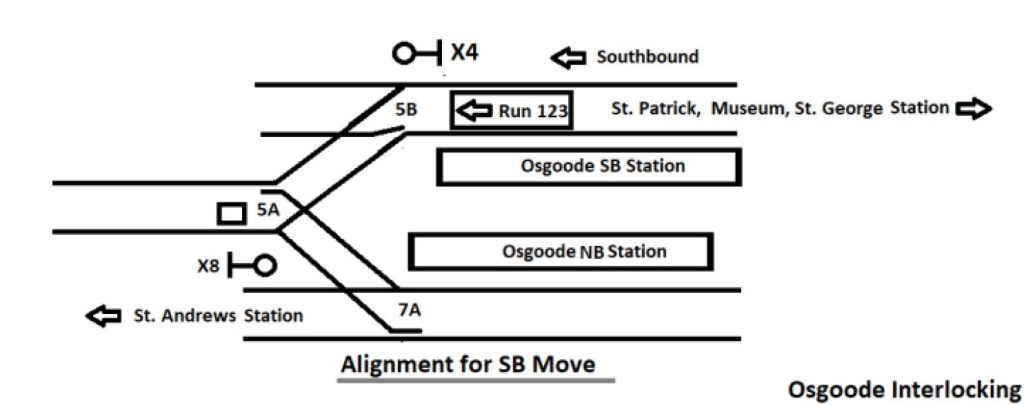
Once run 123 pulled into the pocket, the 5A/5B switches realigned to their normal position for through service southbound. However, this creates a problem on the northbound side as illustrated below. The 5A switch is set for a move out of the pocket to the northbound track, but the 7A switch is aligned for through northbound moves from St. Andrew Station.
This is an inevitable result of a three-into-two track arrangement because under normal operations, both 5B and 7A will be set to the straight for regular operations. Switch 5A will direct an outbound train from the pocket onto one of the mainline tracks unless that move is blocked by some other means through the signal system.
In the pre-ATC system, the train would have been stopped by a “trip arm” at signal X8 that would have tripped emergency brakes. (In the Russell Hill crash in 1995, a trip arm failure contributed to the disaster.) In the ATC system, protection depends on the train being in ATC mode, or if in manual, the movement being carefully managed to avoid conflicts.

One method to protect this track configuration is used at a few exits from pocket tracks, but not all. The south end of the pocket between Lawrence West and Glencairn Stations illustrates this. There are two separate crossovers and switches leading from the pocket track, one each to the northbound and southbound main lines. Each set of switches operates as a pair. During normal mainline operations, both of these would be set leading into a dead-end track in case a train were to move south without being stopped at a signal.

At the north end of this pocket track, there is no comparable setup, and the track arrangement is the same as at Osgoode.

Implementing a dead end track such as at the south end of Lawrence pocket track is difficult to retrofit because there is usually something in the way. This sort of thing must be designed into lines when they are built.
Much of the discussion of this report was in camera and that took roughly an hour and 40 minutes. When the Board returned to public session, it passed two motions. The first was to have a public presentation of the investigation’s findings and the corrective actions taken over the past year at the July 7, 2021 Board meeting. The second was a clear direction that management should inform the Board about serious events at the time they occur.
Chair Jaye Robinson moved “that the TTC Board direct the Chief Executive Officer to alert the Board when an incident meeting the identified thresholds for escalation occurs and subsequently report to the Board once a comprehensive review or investigation has been completed”.
During the Covid era, there has been a gradual slippage of responsibilities from the Board to management as those at the political level have been pre-occupied with city-wide issues. The Board is there to provide oversight and direction, not simply to receive “good news” reports.
Postscript
Ben Spurr’s article on the Board’s actions is here (paywalled).
